Part of the Ortho NI Group
At Shoulder NI, we perform hundreds of procedures every year with consistently high patient satisfaction. With a proven record of effective treatment and recovery management, you can be sure you are in the best of care at Shoulder NI.
Introduction
Introduction
Shoulder Impingement
Frozen Shoulder
Shoulder Dislocation
Chronic Shoulder Instability
Shoulder Arthritis
Introduction
Shoulder Arthroscopy
Rotator Cuff Repair
Shoulder Athroplasty
Shoulder Conditions
Shoulder Procedures
You can be sure you are in the best of care with Ortho NI’s leading shoulder specialists.
The extensive experience of our award-winning consultant, Mr Neill Thompson covers a comprehensive range of orthopaedic procedures.
Shoulder impingement syndrome is pain and often weakness when you raise your arm, caused by a muscle tendon “catching” in your shoulder.
It involves the rotator cuff tendon – a tough, rubbery cord that connects the muscles in your shoulder to the top of your arm. The tendon and muscle run through a narrow space at the top of the shoulder called the subacromial space.

In shoulder impingement syndrome, the tendon becomes trapped in this space and repeatedly scrapes against the bone above, causing pain that tends to be worse when you raise your arm over your head.
You may also experience a persistent ache in your shoulder and pain at night.
Shoulder impingement syndrome can start suddenly after an injury, or (generally from middle age onwards) it can come on gradually without any obvious cause.
What causes shoulder impingement syndrome?
The subacromial space is naturally quite narrow, especially when the arm is raised. Anything that further narrows this space can cause the tendon to become trapped.
Possible causes include:
- bone spurs under the bony roof (acromion) at the top of the subacromial space can narrow the space and catch on the tendon
- swelling or thickening of the rotator cuff tendon – which may result from an injury or general overuse of the shoulder
- inflammation of the fluid-filled sac (bursa) that lies between the rotator cuff tendon and acromion (known as “bursitis”)
- a build-up of calcium deposits within the rotator cuff tendon
Seeking medical advice
See your GP if you have persistent shoulder pain.
They should be able to diagnose shoulder impingement syndrome by asking about your symptoms and examining your shoulder. You may also be asked to do some specific arm movements to help them work out the cause of your pain.
If the cause of your pain is unclear, your GP may refer you for a specialist assessment by a shoulder surgeon, who may also carry out some scans of your shoulder. This can help to rule out other possible causes of shoulder pain.
Treating shoulder impingement syndrome
Caring for your shoulder at home
If shoulder impingement syndrome is only mild, the following measures may be all that are needed:
- Rest the tendon –Avoiding any overarm movements will help prevent any further inflammation (swelling) or damage. Your doctor or physiotherapist will tell you how long you should rest it for, and when you should start exercises (see below).
- Ice packs – Holding an ice pack to the shoulder for around 20 minutes several times a day may help to ease the pain. Don’t put ice directly on your skin – wrap it in a towel. If you don’t have an ice pack, try ice cubes or a bag of frozen vegetables wrapped in a towel.
- Painkillers –Mild non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, can provide short-term pain relief and are available as tablets or a gel that you apply to the shoulder. Other painkillers, such as paracetamol, may also help to ease the pain. If your pain is more severe, a stronger painkiller such as codeine can be prescribed.
Exercises
While it’s important to rest the shoulder joint, you shouldn’t stop movement altogether. Inactivity will cause the muscles to weaken, which will worsen the problem and cause your shoulder to stiffen up. For this reason, a sling is not usually recommended.
Your GP may refer you to a physiotherapist, who will be able to recommend some arm exercises to help stretch and strengthen your shoulder, and improve your range of movement.
After an initial period of supervision by a physiotherapist, you will usually be able to continue doing these exercises at home.
Read more about physiotherapy.
Corticosteroid injections
Corticosteroids are medications that can be used to reduce inflammation and relieve pain. If there is swelling and evidence of inflammation in your shoulder, corticosteroids can be injected directly into the affected area.
They may also be combined with local anaesthetic to further help relieve your pain.
Although corticosteroid injections can relieve pain, without physiotherapy they do not have a long-term effect, and it’s common for the pain to return. You can sometimes have another injection, but you will need to wait at least six weeks. Usually, no more than one to two injections into the same area are recommended.
Possible side effects of corticosteroid injections include thinning and lightening of the skin.
Surgery
If the treatments above aren’t effective, you may need an operation to widen the subacromial space in your shoulder, so the rotator cuff tendon is no longer rubbing against the bone above. This is known as subacromial decompression.
This can usually be done using a technique called arthroscopy, which is a type of keyhole surgery carried out under general anaesthetic, where special surgical instruments and a thin, flexible tube containing a camera are inserted through small cuts in your skin.
This means you should recover faster and with less scarring than if a larger cut was made. Most people are able to go home the same day or the day after.
This technique can also be used to remove any calcium deposits that have formed in the tendon in your shoulder.
Introduction
Frozen shoulder is a condition that leads to pain and stiffness of the shoulder. It’s also known as adhesive capsulitis or shoulder contracture.
The symptoms tend to gradually get worse over a number of months or years. You’ll typically experience shoulder pain for the first two to nine months, which can be severe, followed by increasing stiffness.
The stiffness may affect your ability to carry out everyday activities. In particularly severe cases, you may not be able to move your shoulder at all.
The condition may improve with time, but this can sometimes take several years.
When to see your GP
You should visit your GP if you have persistent shoulder pain that limits your movement.
The earlier frozen shoulder is diagnosed, the more likely it is that treatment can help prevent long-term pain and stiffness.
What causes frozen shoulder?
Frozen shoulder occurs when the flexible tissue that surrounds the shoulder joint, known as the capsule, becomes inflamed and thickened. It’s not fully understood why this happens.
The following can increase your risk of developing a frozen shoulder:
- a previous shoulder injury or shoulder surgery
- diabetes
- Dupuytren’s contracture – a condition where small lumps of thickened tissue form in the hands and fingers
- other health conditions, such as heart disease and stroke
It’s estimated that up to 1 in 20 people in the UK may be affected by frozen shoulder at some point in their life. Most people who get frozen shoulder are between the ages of 40 and 60. The condition is more common in women than men.
How frozen shoulder is treated
Most people with frozen shoulder eventually get better, even without treatment. However, appropriate treatment can help reduce pain and improve the movement in your shoulder until it heals.
The type of treatment you receive will depend on how severe your frozen shoulder is and how far it’s progressed. Possible treatment options include:
- painkillers
- corticosteroid injections
- shoulder exercises
- physiotherapy
If your symptoms haven’t improved after six months, surgery may be recommended
A dislocated shoulder usually happens after a heavy fall onto the arm. It takes between 12 and 16 weeks to heal after the shoulder has been put back into place.
Dislocating your shoulder means the ball joint of your upper arm has popped out of the shoulder socket. The surrounding tissues may also have become overstretched or torn.
The shoulder is one of the easiest joints to dislocate because the ball joint sits in a very shallow socket. This makes the arm extremely mobile and able to move in many directions, but also means it’s not very stable.
Most people dislocate their shoulder during a contact sport such as rugby, or in a sports-related accident. In older people the cause is often falling onto outstretched hands, for example after slipping on ice.
Shoulder dislocations can occur more easily in people who are highy flexible, such as those with joint hypermobility (loose joints).
How do I know if I’ve dislocated my shoulder?
In most cases of dislocated shoulder, the ball part of the joint pops out in front of the shoulder socket. This is usually obvious because:
- you won’t be able to move the arm and it will be extremely painful
- the shoulder will suddenly look square rather than round
- you may be able to see a lump or bulge (the top of the arm bone) under the skin in front of your shoulder
It’s much more unusual for the bone to pop out of the back of the shoulder joint. This usually happens after an epileptic fit or electrocution injury and is less easy to spot.
What you should do
If you think you have dislocated your shoulder, go to your nearest accident and emergency (A&E) department immediately.
Don’t try to pop your arm back in yourself, as this could damage the tissues, nerves and blood vessels around the shoulder joint.
While waiting for medical help, avoid moving your upper arm as much as possible. Place something soft, such as a folded blanket or pillow, in the gap between the arm and side of the chest to support it. If you can, make a simple sling to hold the lower arm across the chest, with the elbow bent at a right angle.
How a dislocated shoulder is treated
When you get to A&E, you will be assessed and examined. You will usually be X-rayed to make sure you haven’t broken any bones, as it’s fairly common for someone who has dislocated their shoulder to also break the bone of their upper arm or the joint.
If you do have a fracture, further scans may also be carried out to investigate it in more detail. Fractures with a shoulder dislocation will require specialist orthopaedic care and may involve surgery.
If you don’t have any fractures, your arm will be gently manipulated back into its shoulder joint using a procedure known as reduction.
Surgery is sometimes necessary if the tissues surrounding the joint are badly torn and the joint is not stable. If the tissues are overstretched but not torn, surgery can sometimes be avoided by doing appropriate exercises to strengthen the shoulder.
Reduction
You will be given some medication to sedate you and ensure you are as relaxed and pain-free as possible.
Reduction is usually carried out in the A&E department, but sometimes it is done in the operating theatre under general anaesthetic (where you are asleep) under the care of an orthopaedic team.
You will usually sit on the bed while the doctor rotates your arm around the shoulder joint until it goes back in its socket. This may take a few minutes.
Once the shoulder joint is back in place, you will often have another X-ray to check the shoulder is in the correct position.
Repairing tears in the shoulder tissues
Some people tear a rotator cuff tendon (bands of tissue that stretch over the top of the shoulder) as well as the labrum (the cuff of tough tissue surrounding and supporting the shoulder joint) when they dislocate their shoulder.
If these tissues have been damaged, you may need surgery to repair them. For some people, this can significantly reduce the risk of dislocating the same shoulder again in the future (see below).
These operations are carried out under general anaesthetic and are increasingly being done with keyhole surgery, using only small incisions and an arthroscope (a thin tube fitted with a light source and a camera).
Recovering from a dislocated shoulder
You can usually go home soon after reduction, but you’ll need to rest your arm in a sling for a few weeks.
You will usually be referred to the orthopaedic department for follow-up care and you may also be referred to a physiotherapist for rehabilitation to strengthen your shoulder.
Arm and shoulder exercises
You may be asked to rest your arm in the sling for two to three weeks while the soft tissues around the shoulder repair themselves.
After this, a physiotherapist can show you some gentle arm and shoulder exercises to do at home with your arm out of its sling. These will help reduce stiffness, relieve some of the pain and build up strength in your shoulder muscles.
Before you begin your exercises, hold an ice pack (or a bag of frozen peas wrapped in a tea towel) on the shoulder for 10 to 15 minutes and take some painkillers.
It’s normal to experience aching, discomfort or stretching when doing these exercises. However, if you have intense pain for more than 30 minutes, do the exercise less forcefully and less often.
It’s better to do short, frequent sessions of five to 10 minutes four times a day rather than one long session, and to gradually increase the number of repetitions you do.
Pain relief
The shoulder may be very painful during the first two to three weeks at home and you may need to take painkillers, such as paracetamol or ibuprofen. Always follow the dosage instructions on the packet.
If this doesn’t control the pain, see your GP for a prescription for a stronger painkiller, such as codeine.
Recovery time
You can stop wearing the sling after a few weeks, but it takes about 12 to 16 weeks to completely recover from a dislocated shoulder.
You can usually resume most activities within two weeks, but avoid heavy lifting and playing sports involving shoulder movements for six weeks to three months. Your orthopaedic surgeon and physiotherapist will advise you.
You’ll probably be off work for two to four weeks, or longer if you have a physical job. Discuss this with your GP, physiotherapist or consultant.
If you’ve also broken your arm or shoulder joint, you may need to wear your sling for up to six weeks and recovery will take longer.
Dislocating the shoulder a second time
If you’ve dislocated your shoulder once, you’re more likely to dislocate it again in the future – particularly if you’re less than 20 years old.
Your chances of another dislocation depend partly on how well the tissues surrounding the joint healed the first time. It can help if the torn tissues were surgically repaired after the dislocated shoulder was fixed.
Regularly doing the exercises your physiotherapist recommends and avoiding awkward arm positions can also reduce the risk of dislocating your shoulder again.
T
he shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This greater range of motion, however, can cause instability.
Shoulder instability occurs when the head of the upper arm bone is forced out of the shoulder socket. This can happen as a result of a sudden injury or from overuse.
Once a shoulder has dislocated, it is vulnerable to repeat episodes. When the shoulder is loose and slips out of place repeatedly, it is called chronic shoulder instability.
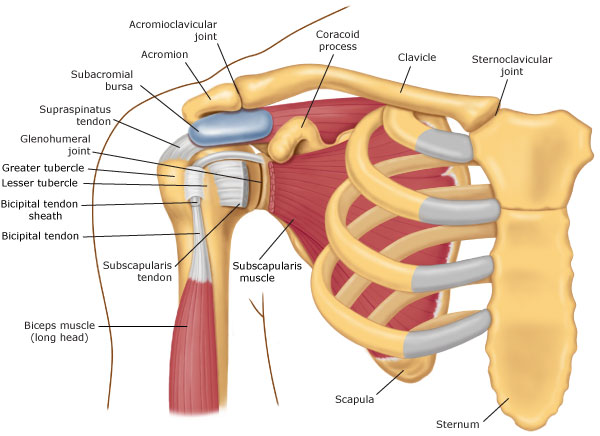
Anatomy

Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head, or ball, of your upper arm bone fits into a shallow socket in your shoulder blade. This socket is called the glenoid. Strong connective tissue, called the shoulder capsule, is the ligament system of the shoulder and keeps the head of the upper arm bone centered in the glenoid socket. This tissue covers the shoulder joint and attaches the upper end of the arm bone to the shoulder blade.
Your shoulder also relies on strong tendons and muscles to keep your shoulder stable.
Description
Shoulder dislocations can be partial, with the ball of the upper arm coming just partially out of the socket. This is called a subluxation. A complete dislocation means the ball comes all the way out of the socket.

Once the ligaments, tendons, and muscles around the shoulder become loose or torn, dislocations can occur repeatedly. Chronic shoulder instability is the persistent inability of these tissues to keep the arm centered in the shoulder socket.auseThere are three common ways that a shoulder can become unstable:
Shoulder Dislocation
Severe injury, or trauma, is often the cause of an initial shoulder dislocation. When the head of the humerus dislocates, the socket bone (glenoid) and the ligaments in the front of the shoulder are often injured. The labrum — the cartilage rim around the edge of the glenoid — may also tear. This is commonly called a Bankart lesion. A severe first dislocation can lead to continued dislocations, giving out, or a feeling of instability.

Repetitive Strain
Some people with shoulder instability have never had a dislocation. Most of these patients have looser ligaments in their shoulders. This increased looseness is sometimes just their normal anatomy. Sometimes, it is the result of repetitive overhead motion.
Swimming, tennis, and volleyball are among the sports requiring repetitive overhead motion that can stretch out the shoulder ligaments. Many jobs also require repetitive overhead work.
Looser ligaments can make it hard to maintain shoulder stability. Repetitive or stressful activities can challenge a weakened shoulder. This can result in a painful, unstable shoulder.
Multidirectional Instability
In a small minority of patients, the shoulder can become unstable without a history of injury or repetitive strain. In such patients, the shoulder may feel loose or dislocate in multiple directions, meaning the ball may dislocate out the front, out the back, or out the bottom of the shoulder. This is called multidirectional instability. These patients have naturally loose ligaments throughout the body and may be “double-jointed.”
Common symptoms of chronic shoulder instability include:
- Pain caused by shoulder injury
- Repeated shoulder dislocations
- Repeated instances of the shoulder giving out
- A persistent sensation of the shoulder feeling loose, slipping in and out of the joint, or just “hanging there”
Physical Examination and Patient History
After discussing your symptoms and medical history, your doctor will examine your shoulder. Specific tests help your doctor assess instability in your shoulder. Your doctor may also test for general looseness in your ligaments. For example, you may be asked to try to touch your thumb to the underside of your forearm.
Imaging Tests
Your doctor may order imaging tests to help confirm your diagnosis and identify any other problems.
X-rays. These pictures will show any injuries to the bones that make up your shoulder joint.
Magnetic resonance imaging (MRI). This provides detailed images of soft tissues. It may help your doctor identify injuries to the ligaments and tendons surrounding your shoulder joint.
Chronic shoulder instability is often first treated with nonsurgical options. If these options do not relieve the pain and instability, surgery may be needed.
Nonsurgical Treatment
Your doctor will develop a treatment plan to relieve your symptoms. It often takes several months of nonsurgical treatment before you can tell how well it is working. Nonsurgical treatment typically includes:
Activity modification. You must make some changes in your lifestyle and avoid activities that aggravate your symptoms.
Non-steroidal anti-inflammatory medication. Drugs like aspirin and ibuprofen reduce pain and swelling.
Physical therapy. Strengthening shoulder muscles and working on shoulder control can increase stability. Your therapist will design a home exercise program for your shoulder.
Surgical Treatment
Surgery is often necessary to repair torn or stretched ligaments so that they are better able to hold the shoulder joint in place.

Arthroscopy. Soft tissues in the shoulder can be repaired using tiny instruments and small incisions. This is a same-day or outpatient procedure. Arthroscopy is a minimally invasive surgery. Your surgeon will look inside the shoulder with a tiny camera and perform the surgery with special pencil-thin instruments.
Open Surgery. Some patients may need an open surgical procedure. This involves making a larger incision over the shoulder and performing the repair under direct visualization.
Rehabilitation. After surgery, your shoulder may be immobilized temporarily with a sling.
When the sling is removed, exercises to rehabilitate the ligaments will be started. These will improve the range of motion in your shoulder and prevent scarring as the ligaments heal. Exercises to strengthen your shoulder will gradually be added to your rehabilitation plan.
Be sure to follow your doctor’s treatment plan. Although it is a slow process, your commitment to physical therapy is the most important factor in returning to all the activities you enjoy.
The shoulder is the most moveable joint in your body. It helps you to lift your arm, to rotate it, and to reach up over your head. It is able to turn in many directions. This greater range of motion, however, can cause instability.
Shoulder instability occurs when the head of the upper arm bone is forced out of the shoulder socket. This can happen as a result of a sudden injury or from overuse.
Once a shoulder has dislocated, it is vulnerable to repeat episodes. When the shoulder is loose and slips out of place repeatedly, it is called chronic shoulder instability.
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head, or ball, of your upper arm bone fits into a shallow socket in your shoulder blade. This socket is called the glenoid. Strong connective tissue, called the shoulder capsule, is the ligament system of the shoulder and keeps the head of the upper arm bone centered in the glenoid socket. This tissue covers the shoulder joint and attaches the upper end of the arm bone to the shoulder blade.
Your shoulder also relies on strong tendons and muscles to keep your shoulder stable.
Description
Shoulder dislocations can be partial, with the ball of the upper arm coming just partially out of the socket. This is called a subluxation. A complete dislocation means the ball comes all the way out of the socket.
Once the ligaments, tendons, and muscles around the shoulder become loose or torn, dislocations can occur repeatedly. Chronic shoulder instability is the persistent inability of these tissues to keep the arm centered in the shoulder socket.
Cause
There are three common ways that a shoulder can become unstable:
Shoulder Dislocation
Severe injury, or trauma, is often the cause of an initial shoulder dislocation. When the head of the humerus dislocates, the socket bone (glenoid) and the ligaments in the front of the shoulder are often injured. The labrum — the cartilage rim around the edge of the glenoid — may also tear. This is commonly called a Bankart lesion. A severe first dislocation can lead to continued dislocations, giving out, or a feeling of instability.
Repetitive Strain
Some people with shoulder instability have never had a dislocation. Most of these patients have looser ligaments in their shoulders. This increased looseness is sometimes just their normal anatomy. Sometimes, it is the result of repetitive overhead motion.
Swimming, tennis, and volleyball are among the sports requiring repetitive overhead motion that can stretch out the shoulder ligaments. Many jobs also require repetitive overhead work.
Looser ligaments can make it hard to maintain shoulder stability. Repetitive or stressful activities can challenge a weakened shoulder. This can result in a painful, unstable shoulder.
Multidirectional Instability
In a small minority of patients, the shoulder can become unstable without a history of injury or repetitive strain. In such patients, the shoulder may feel loose or dislocate in multiple directions, meaning the ball may dislocate out the front, out the back, or out the bottom of the shoulder. This is called multidirectional instability. These patients have naturally loose ligaments throughout the body and may be “double-jointed.”
Symptoms
Common symptoms of chronic shoulder instability include:
- Pain caused by shoulder injury
- Repeated shoulder dislocations
- Repeated instances of the shoulder giving out
- A persistent sensation of the shoulder feeling loose, slipping in and out of the joint, or just “hanging there”
Physical Examination and Patient History
After discussing your symptoms and medical history, your doctor will examine your shoulder. Specific tests help your doctor assess instability in your shoulder. Your doctor may also test for general looseness in your ligaments. For example, you may be asked to try to touch your thumb to the underside of your forearm.
Imaging Tests
Your doctor may order imaging tests to help confirm your diagnosis and identify any other problems.
X-rays. These pictures will show any injuries to the bones that make up your shoulder joint.
Magnetic resonance imaging (MRI). This provides detailed images of soft tissues. It may help your doctor identify injuries to the ligaments and tendons surrounding your shoulder joint.
TreatmentChronic shoulder instability is often first treated with nonsurgical options. If these options do not relieve the pain and instability, surgery may be needed.
Nonsurgical Treatment
Your doctor will develop a treatment plan to relieve your symptoms. It often takes several months of nonsurgical treatment before you can tell how well it is working. Nonsurgical treatment typically includes:
Activity modification. You must make some changes in your lifestyle and avoid activities that aggravate your symptoms.
Non-steroidal anti-inflammatory medication. Drugs like aspirin and ibuprofen reduce pain and swelling.
Physical therapy. Strengthening shoulder muscles and working on shoulder control can increase stability. Your therapist will design a home exercise program for your shoulder.
Surgical Treatment
Surgery is often necessary to repair torn or stretched ligaments so that they are better able to hold the shoulder joint in place.
Arthroscopy. Soft tissues in the shoulder can be repaired using tiny instruments and small incisions. This is a same-day or outpatient procedure. Arthroscopy is a minimally invasive surgery. Your surgeon will look inside the shoulder with a tiny camera and perform the surgery with special pencil-thin instruments.
Open Surgery. Some patients may need an open surgical procedure. This involves making a larger incision over the shoulder and performing the repair under direct visualization.
Rehabilitation. After surgery, your shoulder may be immobilized temporarily with a sling.
When the sling is removed, exercises to rehabilitate the ligaments will be started. These will improve the range of motion in your shoulder and prevent scarring as the ligaments heal. Exercises to strengthen your shoulder will gradually be added to your rehabilitation plan.
Be sure to follow your doctor’s treatment plan. Although it is a slow process, your commitment to physical therapy is the most important factor in returning to all the activities you enjoy.
Simply defined, arthritis is inflammation of one or more of your joints. In a diseased shoulder, inflammation causes pain and stiffness.
Although there is no cure for arthritis of the shoulder, there are many treatment options available. Using these, most people with arthritis are able to manage pain and stay active.

Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. A combination of muscles and tendons keeps your arm bone centered in your shoulder socket. These tissues are called the rotator cuff.
There are two joints in the shoulder, and both may be affected by arthritis. One joint is located where the clavicle meets the tip of the shoulder blade (acromion). This is called the acromioclavicular (AC) joint.
Where the head of the humerus fits into the scapula is called the glenohumeral joint.
To provide you with effective treatment, your physician will need to determine which joint is affected and what type of arthritis you have.
Description
Five major types of arthritis typically affect the shoulder.
Osteoarthritis
Also known as “wear-and-tear” arthritis, osteoarthritis is a condition that destroys the smooth outer covering (articular cartilage) of bone. As the cartilage wears away, it becomes frayed and rough, and the protective space between the bones decreases. During movement, the bones of the joint rub against each other, causing pain.
Osteoarthritis usually affects people over 50 years of age and is more common in the acromioclavicular joint than in the glenohumeral shoulder joint.

Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a chronic disease that attacks multiple joints throughout the body. It is symmetrical, meaning that it usually affects the same joint on both sides of the body.
The joints of your body are covered with a lining — called synovium — that lubricates the joint and makes it easier to move. Rheumatoid arthritis causes the lining to swell, which causes pain and stiffness in the joint.
Rheumatoid arthritis is an autoimmune disease. This means that the immune system attacks its own tissues. In RA, the defenses that protect the body from infection instead damage normal tissue (such as cartilage and ligaments) and soften bone.
Rheumatoid arthritis is equally common in both joints of the shoulder.
Post-traumatic Arthritis
Posttraumatic arthritis is a form of osteoarthritis that develops after an injury, such as a fracture or dislocation of the shoulder.
Rotator Cuff Tear Arthropathy

Arthritis can also develop after a large, long-standing rotator cuff tendon tear. The torn rotator cuff can no longer hold the head of the humerus in the glenoid socket, and the humerus can move upward and rub against the acromion. This can damage the surfaces of the bones, causing arthritis to develop.
The combination of a large rotator cuff tear and advanced arthritis can lead to severe pain and weakness, and the patient may not be able to lift the arm away from the side.
Avascular Necrosis
Avascular necrosis (AVN) of the shoulder is a painful condition that occurs when the blood supply to the head of the humerus is disrupted. Because bone cells die without a blood supply, AVN can ultimately lead to destruction of the shoulder joint and arthritis.
Avascular necrosis develops in stages. As it progresses, the dead bone gradually collapses, which damages the articular cartilage covering the bone and leads to arthritis. At first, AVN affects only the head of the humerus, but as AVN progresses, the collapsed head of the humerus can damage the glenoid socket.
Causes of AVN include high dose steroid use, heavy alcohol consumption, sickle cell disease, and traumatic injury, such as fractures of the shoulder. In some cases, no cause can be identified; this is referred to as idiopathic AVN.
Symptoms
Pain. The most common symptom of arthritis of the shoulder is pain, which is aggravated by activity and progressively worsens.
- If the glenohumeral shoulder joint is affected, the pain is centered in the back of the shoulder and may intensify with changes in the weather. Patients complain of an ache deep in the joint.
- The pain of arthritis in the acromioclavicular (AC) joint is focused on the top of the shoulder. This pain can sometimes radiate or travel to the side of the neck.
- Someone with rheumatoid arthritis may have pain throughout the shoulder if both the glenohumeral and AC joints are affected.
Limited range of motion. Limited motion is another common symptom. It may become more difficult to lift your arm to comb your hair or reach up to a shelf. You may hear a grinding, clicking, or snapping sound (crepitus) as you move your shoulder.
As the disease progresses, any movement of the shoulder causes pain. Night pain is common and sleeping may be difficult.
Examination
Medical History and Physical Examination
After discussing your symptoms and medical history, your doctor will examine your shoulder.
During the physical examination, your doctor will look for:
- Weakness (atrophy) in the muscles
- Tenderness to touch
- Extent of passive (assisted) and active (self-directed) range of motion
- Any signs of injury to the muscles, tendons, and ligaments surrounding the joint
- Signs of previous injuries
- Involvement of other joints (an indication of rheumatoid arthritis)
- Crepitus (a grating sensation inside the joint) with movement
- Pain when pressure is placed on the joint
X-Rays
X-rays are imaging tests that create detailed pictures of dense structures, like bone. They can help distinguish among various forms of arthritis.
X-rays of an arthritic shoulder will show a narrowing of the joint space, changes in the bone, and the formation of bone spurs (osteophytes).

To confirm the diagnosis, your doctor may inject a local anaesthetic into the joint. If it temporarily relieves the pain, the diagnosis of arthritis is supported.
Treatment
Nonsurgical Treatment
As with other arthritic conditions, initial treatment of arthritis of the shoulder is nonsurgical. Your doctor may recommend the following treatment options:
- Rest or change in activities to avoid provoking pain. You may need to change the way you move your arm to do things.
- Physical therapy exercises may improve the range of motion in your shoulder.
- Nonsteroidal anti-inflammatory medications (NSAIDs), such as aspirin or ibuprofen, may reduce inflammation and pain. These medications can irritate the stomach lining and cause internal bleeding. They should be taken with food. Consult with your doctor before taking over-the-counter NSAIDs if you have a history of ulcers or are taking blood thinning medication.
- Corticosteroid injections in the shoulder can dramatically reduce the inflammation and pain. However, the effect is often temporary.
- Moist heat
- Ice your shoulder for 20 to 30 minutes two or three times a day to reduce inflammation and ease pain.
- If you have rheumatoid arthritis, your doctor may prescribe a disease-modifying drug, such as methotrexate.
- Dietary supplements, such as glucosamine and chondroitin sulfate may help relieve pain. (Note: There is little scientific evidence to support the use of glucosamine and chondroitin sulfate to treat arthritis. In addition, the U.S. Food and Drug Administration does not test dietary supplements. These compounds may cause negative interactions with other medications. Always consult your doctor before taking dietary supplements.)
Surgical Treatment
Your doctor may consider surgery if your pain causes disability and is not relieved with nonsurgical options.
Arthroscopy. Cases of mild glenohumeral arthritis may be treated with arthroscopy, During arthroscopy, the surgeon inserts a small camera, called an arthroscope, into the shoulder joint. The camera displays pictures on a television screen, and the surgeon uses these images to guide miniature surgical instruments.
Because the arthroscope and surgical instruments are thin, the surgeon can use very small incisions (cuts), rather than the larger incision needed for standard, open surgery.
During the procedure, your surgeon can debride (clean out) the inside of the joint. Although the procedure provides pain relief, it will not eliminate the arthritis from the joint. If the arthritis progresses, further surgery may be needed in the future.
Shoulder joint replacement (arthroplasty). Advanced arthritis of the glenohumeral joint can be treated with shoulder replacement surgery, in which the damaged parts of the shoulder are removed and replaced with artificial components, called a prosthesis.

Replacement surgery options include:
- Hemiarthroplasty. Just the head of the humerus is replaced by an artificial component.
- Total shoulder arthroplasty. Both the head of the humerus and the glenoid are replaced. A plastic “cup” is fitted into the glenoid, and a metal “ball” is attached to the top of the humerus.
- Reverse total shoulder arthroplasty. In a reverse total shoulder replacement, the socket and metal ball are opposite a conventional total shoulder arthroplasty. The metal ball is fixed to the glenoid and the plastic cup is fixed to the upper end of the humerus. A reverse total shoulder replacement works better for people with cuff tear arthropathy because it relies on different muscles — not the rotator cuff — to move the arm.
Resection arthroplasty. The most common surgical procedure used to treat arthritis of the acromioclavicular joint is a resection arthroplasty. Your surgeon may choose to do this arthroscopically.
In this procedure, a small amount of bone from the end of the collarbone is removed, leaving a space that gradually fills in with scar tissue.
Recovery. Surgical treatment of arthritis of the shoulder is generally very effective in reducing pain and restoring motion. Recovery time and rehabilitation plans depend upon the type of surgery performed.
Pain management. After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Complications. As with all surgeries, there are some risks and possible complications. Potential problems after shoulder surgery include infection, excessive bleeding, blood clots, and damage to blood vessels or nerves.
Your surgeon will discuss the possible complications with you before your operation.
At Ortho-NI we provide high quality healthcare with years of experience in treating life altering painful conditions with a goal of obtaining pain-free high functioning quality of life.
Arthroscopy is a procedure that orthopaedic surgeons use to inspect, diagnose, and repair problems inside a joint.
The word arthroscopy comes from two Greek words, “arthro” (joint) and “skopein” (to look). The term literally means “to look within the joint.” During shoulder arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your shoulder joint. The camera displays pictures on a television screen, and your surgeon uses these images to guide miniature surgical instruments.
Because the arthroscope and surgical instruments are thin, your surgeon can use very small incisions (cuts), rather than the larger incision needed for standard, open surgery. This results in less pain for patients, and shortens the time it takes to recover and return to favorite activities.
Anatomy
Your shoulder is a complex joint that is capable of more motion than any other joint in your body. It is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
Ball and socket. The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. A slippery tissue called articular cartilage covers the surface of the ball and the socket. It creates a smooth, frictionless surface that helps the bones glide easily across each other.
The glenoid is ringed by strong fibrous cartilage called the labrum. The labrum forms a gasket around the socket, adds stability, and cushions the joint.
Shoulder capsule. The joint is surrounded by bands of tissue called ligaments. They form a capsule that holds the joint together. The undersurface of the capsule is lined by a thin membrane called the synovium. It produces synovial fluid that lubricates the shoulder joint.
Rotator cuff. Four tendons surround the shoulder capsule and help keep your arm bone centered in your shoulder socket. This thick tendon material is called the rotator cuff. The cuff covers the head of the humerus and attaches it to your shoulder blade.
Bursa. There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa helps the rotator cuff tendons glide smoothly when you move your arm.

When Shoulder Arthroscopy Is Recommended
Your doctor may recommend shoulder arthroscopy if you have a painful condition that does not respond to nonsurgical treatment. Nonsurgical treatment includes rest, physical therapy, and medications or injections that can reduce inflammation. Inflammation is one of your body’s normal reactions to injury or disease. In an injured or diseased shoulder joint, inflammation causes swelling, pain, and stiffness.
Injury, overuse, and age-related wear and tear are responsible for most shoulder problems. Shoulder arthroscopy may relieve painful symptoms of many problems that damage the rotator cuff tendons, labrum, articular cartilage, and other soft tissues surrounding the joint.
Common arthroscopic procedures include:
- Rotator cuff repair
- Bone spur removal
- Removal or repair of the labrum
- Repair of ligaments
- Removal of inflamed tissue or loose cartilage
- Repair for recurrent shoulder dislocation
Less common procedures such as nerve release, fracture repair, and cyst excision can also be performed using an arthroscope. Some surgical procedures, such as shoulder replacement, still require open surgery with more extensive incisions.

Planning for Surgery
Your orthopaedic surgeon may ask you to see your primary doctor to make sure that you do not have any medical problems that need to be addressed before your surgery. Blood tests, an electrocardiogram, or chest x-ray may be needed to safely perform your surgery.
If you have certain health risks, a more extensive evaluation may be necessary before your surgery. Be sure to inform your orthopaedic surgeon of any medications or supplements that you take. You may need to stop taking some of these prior to surgery.
If you are generally healthy, your arthroscopy will most likely be performed as an outpatient. This means you will not need to stay overnight at the hospital.
The hospital or surgery center will contact you ahead of time to provide specific details about your procedure. Make sure to follow the instructions on when to arrive and especially on when to stop eating or drinking prior to your surgery.
Before the operation, a member of the anesthesia staff will talk with you about anesthesia options. Shoulder arthroscopy is most commonly performed using regional nerve blocks which numb your shoulder and arm. This numbing medicine is injected in the base of your neck or high on your shoulder. This is where the nerves that control feeling in your shoulder and arm are located. In addition to its use as an anesthetic during surgery, a nerve block will help control pain for a few hours after the surgery is completed. Many surgeons combine nerve blocks with sedation or a light general anesthetic because patients can become uncomfortable staying in one position for the length of time needed to complete the surgery.
Most arthroscopic procedures take less than an hour, however, the length of your surgery will depend on what your surgeon finds and what repairs are required.
Surgical Procedure
Positioning and Preparation
Once in the operating room, you will be positioned so that your surgeon can easily adjust the arthroscope to have a clear view of the inside of your shoulder. The two most common patient positions for arthroscopic shoulder surgery are:
- Beach chair position. This is a semi-seated position similar to sitting in a reclining chair.
- Lateral decubitius position. In this position the patient lies on his or her side on an operating table.
Each position has some slight advantages. Surgeons select positions based on the procedure being performed, as well as their individual training.
Once you are positioned, the surgical team will remove hair, if needed, and then spread an antiseptic solution over your shoulder to clean the skin. They will cover your shoulder and arm with sterile drapes, and will most likely place your forearm in a holding device to ensure your arm stays still.
Procedure
Your surgeon will first inject fluid into the shoulder to inflate the joint. This makes it easier to see all the structures of your shoulder through the arthroscope. Then your surgeon will make a small puncture in your shoulder (about the size of a buttonhole) for the arthroscope. Fluid flows through the arthroscope to keep the view clear and control any bleeding. Images from the arthroscope are projected on the video screen showing your surgeon the inside of your shoulder and any damage.

Once the problem is clearly identified, your surgeon will insert other small instruments through separate incisions to repair it. Specialized instruments are used for tasks like shaving, cutting, grasping, suture passing, and knot tying. In many cases, special devices are used to anchor stitches into bone.


Your surgeon may close your incisions with stitches or steri-strips (small paper sutures) and cover them with a large, soft bandage.
Recovery
Postoperative
After surgery, you will stay in the recovery room for 1 to 2 hours before being discharged home. Nurses will monitor your responsiveness and provide pain medication, if needed. You will need someone to drive you home and stay with you for at least the first night.
At Home
Although recovery from arthroscopy is often faster than recovery from open surgery, it may still take weeks for your shoulder joint to completely recover.
You can expect some pain and discomfort for at least a week after surgery. If you have had a more extensive surgery, however, it may take several weeks before your pain subsides. Ice will help relieve pain and swelling. Your doctor may prescribe pain medicine, if needed.
Although it does not affect how your shoulder heals, lying flat may pull on your shoulder and cause discomfort. Some patients are more comfortable sleeping in a reclining chair or propped up in bed during the first days after surgery.
A few days after surgery, you should be able to replace your large bandage with simple Band-Aids. You may shower once your wounds are no longer draining, but try not to soak or scrub your incisions.
You will most likely need a sling or special immobilizer to protect your shoulder. Your surgeon will discuss with you how long the sling will be needed.
Rehabilitation
Rehabilitation plays an important role in getting you back to your daily activities. An exercise program will help you regain shoulder strength and motion. Your surgeon will develop a rehabilitation plan based on the surgical procedures you required.
If you have had a more complicated surgical repair, your surgeon may recommend a physical therapist to supervise your exercise program.
It is important that you make a strong effort at rehabilitation in order for your surgery to succeed.
Complications
Most patients do not experience complications from shoulder arthroscopy. As with any surgery, however, there are some risks. These are usually minor and treatable. Potential problems with arthroscopy include infection, excessive bleeding, blood clots, and damage to blood vessels or nerves.
Your surgeon will discuss the possible complications with you before your operation.
Rotator Cuff Tears: Surgical Treatment Options
Surgery to repair a torn rotator cuff most often involves re-attaching the tendon to the head of humerus (upper arm bone). A partial tear, however, may need only a trimming or smoothing procedure called a debridement. A complete tear within the thickest part of the tendon is repaired by stitching the two sides back together.
When is Rotator Cuff Repair Recommended?
Your doctor may recommend surgery for a torn rotator cuff if your pain does not improve with nonsurgical methods. Continued pain is the main indication for surgery. If you are very active and use your arms for overhead work or sports, your doctor may also suggest surgery.
Other signs that surgery may be a good option for you include:
- Your symptoms have lasted 6 to 12 months
- You have a large tear (more than 3 cm)
- You have significant weakness and loss of function in your shoulder
- Your tear was caused by a recent, acute injury

There are a few options for repairing rotator cuff tears. Advancements in surgical techniques for rotator cuff repair include less invasive procedures. While each of the methods available has its own advantages and disadvantages, all have the same goal: getting the tendon to heal.
The type of repair performed depends on several factors, including your surgeon’s experience and familiarity with a particular procedure, the size of your tear, your anatomy, and the quality of the tendon tissue and bone.
Many surgical repairs can be done on an outpatient basis and do not require you to stay overnight in the hospital. Your orthopaedic surgeon will discuss with you the best procedure to meet your individual health needs.
You may have other shoulder problems in addition to a rotator cuff tear, such as osteoarthritis, bone spurs, or other soft tissue tears. During the operation, your surgeon may be able to take care of these problems, as well.
The three techniques most commonly used for rotator cuff repair include traditional open repair, arthroscopic repair, and mini-open repair. In the end, patients rate all three repair methods the same for pain relief, strength improvement, and overall satisfaction.
Open Repair
A traditional open surgical incision (several centimeters long) is often required if the tear is large or complex. The surgeon makes the incision over the shoulder and detaches the shoulder muscle (deltoid) to better see and gain access to the torn tendon.
During an open repair, the surgeon typically removes bone spurs from the underside of the acromion (this procedure is called an acromioplasty). An open repair may be a good option if the tear is large or complex or if additional reconstruction, such as a tendon transfer, is indicated.
Open repair was the first technique used for torn rotator cuffs. Over the years, new technology and improved surgeon experience has led to less invasive procedures.
All-Arthroscopic Repair
During arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your shoulder joint. The camera displays pictures on a television screen, and your surgeon uses these images to guide miniature surgical instruments.
Because the arthroscope and surgical instruments are thin, your surgeon can use very small incisions (cuts), rather than the larger incision needed for standard, open surgery.
All-arthroscopic repair is usually an outpatient procedure and is the least invasive method to repair a torn rotator cuff.

Mini-Open Repair
The mini-open repair uses newer technology and instruments to perform a repair through a small incision. The incision is typically 3 to 5 cm long.
This technique uses arthroscopy to assess and treat damage to other structures within the joint. Bone spurs, for example, are often removed arthroscopically. This avoids the need to detach the deltoid muscle.
Once the arthroscopic portion of the procedure is completed, the surgeon repairs the rotator cuff through the mini-open incision. During the tendon repair, the surgeon views the shoulder structures directly, rather than through the video monitor.
Recovery
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Rehabilitation
Rehabilitation plays a vital role in getting you back to your daily activities. A physical therapy program will help you regain shoulder strength and motion.
Immobilization. After surgery, therapy progresses in stages. At first, the repair needs to be protected while the tendon heals. To keep your arm from moving, you will most likely use a sling and avoid using your arm for the first 4 to 6 weeks. How long you require a sling depends upon the severity of your injury.
Passive exercise. Even though your tear has been repaired, the muscles around your arm remain weak. Once your surgeon decides it is safe for you to move your arm and shoulder, a therapist will help you with passive exercises to improve range of motion in your shoulder. With passive exercise, your therapist supports your arm and moves it in different positions. In most cases, passive exercise is begun within the first 4 to 6 weeks after surgery.
Active exercise. After 4 to 6 weeks, you will progress to doing active exercises without the help of your therapist. Moving your muscles on your own will gradually increase your strength and improve your arm control. At 8 to 12 weeks, your therapist will start you on a strengthening exercise program.
Expect a complete recovery to take several months. Most patients have a functional range of motion and adequate strength by 4 to 6 months after surgery. Although it is a slow process, your commitment to rehabilitation is key to a successful outcome.
Outcome
The majority of patients report improved shoulder strength and less pain after surgery for a torn rotator cuff.
Each surgical repair technique (open, mini-open, and arthroscopic) has similar results in terms of pain relief, improvement in strength and function, and patient satisfaction. Surgeon expertise is more important in achieving satisfactory results than the choice of technique.
Factors that can decrease the likelihood of a satisfactory result include:
- Poor tendon/tissue quality
- Large or massive tears
- Poor patient compliance with rehabilitation and restrictions after surgery
- Patient age (older than 65 years)
- Smoking and use of other nicotine products
- Workers’ compensation claims
Complications
- Nerve injury. This typically involves the nerve that activates your shoulder muscle (deltoid).
- Infection. Patients are given antibiotics during the procedure to lessen the risk for infection. If an infection develops, an additional surgery or prolonged antibiotic treatment may be needed.
- Deltoid detachment. During an open repair, this shoulder muscle is detached to provide better access to the rotator cuff. It is stitched back into place at the end of the procedure. It is very important to protect this area after surgery and during rehabilitation to allow it to heal.
- Stiffness. Early rehabilitation lessens the likelihood of permanent stiffness or loss of motion. Most of the time, stiffness will improve with more aggressive therapy and exercise.
- Tendon re-tear. There is a chance for re-tear following all types of repairs. The larger the tear, the higher the risk of re-tear. Patients who re-tear their tendons usually do not have greater pain or decreased shoulder function. Repeat surgery is needed only if there is severe pain or loss of function.
Shoulder Joint Replacement
Although shoulder joint replacement is less common than knee or hip replacement, it is just as successful in relieving joint pain.
Shoulder replacement surgery was first performed in the 1950s to treat severe shoulder fractures. Over the years, shoulder joint replacement has come to be used for many other painful conditions of the shoulder, such as different forms of arthritis.
If nonsurgical treatments like medications and activity changes are no longer helpful for relieving pain, you may want to consider shoulder joint replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain and help you resume everyday activities.
Whether you have just begun exploring treatment options or have already decided to have shoulder joint replacement surgery, this article will help you understand more about this valuable procedure.
Anatomy
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle). The shoulder is a ball-and-socket joint: The ball, or head, of your upper arm bone fits into a shallow socket in your shoulder blade. This socket is called the glenoid.
The surfaces of the bones where they touch are covered with articular cartilage, a smooth substance that protects the bones and enables them to move easily. A thin, smooth tissue called synovial membrane covers all remaining surfaces inside the shoulder joint. In a healthy shoulder, this membrane makes a small amount of fluid that lubricates the cartilage and eliminates almost any friction in your shoulder.
The muscles and tendons that surround the shoulder provide stability and support.
All of these structures allow the shoulder to rotate through a greater range of motion than any other joint in the body.

Description
In shoulder replacement surgery, the damaged parts of the shoulder are removed and replaced with artificial components, called a prosthesis. The treatment options are either replacement of just the head of the humerus bone (ball), or replacement of both the ball and the socket (glenoid).
Cause
Several conditions can cause shoulder pain and disability, and lead patients to consider shoulder joint replacement surgery.
Osteoarthritis (Degenerative Joint Disease)
This is an age-related “wear and tear” type of arthritis. It usually occurs in people 50 years of age and older, but may occur in younger people, too. The cartilage that cushions the bones of the shoulder softens and wears away. The bones then rub against one another. Over time, the shoulder joint slowly becomes stiff and painful.
Unfortunately, there is no way to prevent the development of osteoarthritis. It is a common reason people have shoulder replacement surgery.

Rheumatoid Arthritis
This is a disease in which the synovial membrane that surrounds the joint becomes inflamed and thickened. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness. Rheumatoid arthritis is the most common form of a group of disorders termed “inflammatory arthritis.”
Post-traumatic Arthritis
This can follow a serious shoulder injury. Fractures of the bones that make up the shoulder or tears of the shoulder tendons or ligaments may damage the articular cartilage over time. This causes shoulder pain and limits shoulder function.
Rotator Cuff Tear Arthropathy
A patient with a very large, long-standing rotator cuff tear may develop cuff tear arthropathy. In this condition, the changes in the shoulder joint due to the rotator cuff tear may lead to arthritis and destruction of the joint cartilage.
Avascular Necrosis (Osteonecrosis)
Avascular necrosis is a painful condition that occurs when the blood supply to the bone is disrupted. Because bone cells die without a blood supply, osteonecrosis can ultimately cause destruction of the shoulder joint and lead to arthritis. Chronic steroid use, deep sea diving, severe fracture of the shoulder, sickle cell disease, and heavy alcohol use are risk factors for avascular necrosis.
Severe Fractures
A severe fracture of the shoulder is another common reason people have shoulder replacements. When the head of the upper arm bone is shattered, it may be very difficult for a doctor to put the pieces of bone back in place. In addition, the blood supply to the bone pieces can be interrupted. In this case, a surgeon may recommend a shoulder replacement. Older patients with osteoporosis are most at risk for severe shoulder fractures.
Failed Previous Shoulder Replacement Surgery
Although uncommon, some shoulder replacements fail, most often because of implant loosening, wear, infection, and dislocation. When this occurs, a second joint replacement surgery — called a revision surgery — may be necessary.
There are several reasons why your doctor may recommend shoulder replacement surgery. People who benefit from surgery often have:
- Severe shoulder pain that interferes with everyday activities, such as reaching into a cabinet, dressing, toileting, and washing.
- Moderate to severe pain while resting. This pain may be severe enough to prevent a good night’s sleep.
- Loss of motion and/or weakness in the shoulder.
- Failure to substantially improve with other treatments such as anti-inflammatory medications, cortisone injections, or physical therapy.
Your family physician may refer you to an orthopaedic surgeon for a thorough evaluation to determine if you can benefit from this surgery.
An evaluation with an orthopaedic surgeon consists of several components:
- A medical history. Your orthopaedic surgeon will gather information about your general health and ask you about the extent of your shoulder pain and your ability to function.
- A physical examination. This will assess shoulder motion, stability, and strength.
- X-rays. These images help to determine the extent of damage in your shoulder. They can show loss of the normal joint space between bones, flattening or irregularity in the shape of the bone, bone spurs, and loose pieces of cartilage or bone that may be floating inside the joint.
- Other tests. Occasionally blood tests, a magnetic resonance imaging (MRI) scan, or a bone scan may be needed to determine the condition of the bone and soft tissues of your shoulder.

Your orthopaedic surgeon will review the results of your evaluation with you and discuss whether shoulder joint replacement is the best method to relieve your pain and improve your function. Other treatment options — including medications, injections, physical therapy, or other types of surgery — will also be discussed and considered.
Shoulder Replacement Options
Shoulder replacement surgery is highly technical. It should be performed by a surgical team with experience in this procedure.
There are different types of shoulder replacements. Your surgeon will evaluate your situation carefully before making any decisions. He or she will discuss with you which type of replacement would best meet your health needs. Do not hesitate to ask what type of implant will be used in your situation, and why that choice is right for you.
Total Shoulder Replacement
The typical total shoulder replacement involves replacing the arthritic joint surfaces with a highly polished metal ball attached to a stem, and a plastic socket.

These components come in various sizes. They may be either cemented or “press fit” into the bone. If the bone is of good quality, your surgeon may choose to use a non-cemented (press-fit) humeral component. If the bone is soft, the humeral component may be implanted with bone cement. In most cases, an all-plastic glenoid (socket) component is implanted with bone cement.
Implantation of a glenoid component is not advised if:
- The glenoid has good cartilage
- The glenoid bone is severely deficient
- The rotator cuff tendons are irreparably torn
Patients with bone-on-bone osteoarthritis and intact rotator cuff tendons are generally good candidates for conventional total shoulder replacement.

Stemmed Hemiarthroplasty
Depending on the condition of your shoulder, your surgeon may replace only the ball. This procedure is called a hemiarthroplasty. In a traditional hemiarthroplasty, the head of the humerus is replaced with a metal ball and stem, similar to the component used in a total shoulder replacement. This is called a stemmed hemiarthroplasty.
Some surgeons recommend hemiarthroplasty when the humeral head is severely fractured but the socket is normal. Other indications for a hemiarthroplasty include:
- Arthritis that only involves the head of the humerus with a glenoid that has a healthy and intact cartilage surface
- Shoulders with severely weakened bone in the glenoid
- Some shoulders with severely torn rotator cuff tendons and arthritis
Sometimes, surgeons make the decision between a total shoulder replacement and a hemiarthroplasty in the operating room at the time of the surgery.
Studies show that patients with osteoarthritis get better pain relief from total shoulder arthroplasty than from hemiarthroplasty.
Resurfacing Hemiarthroplasty
Resurfacing hemiarthroplasty involves replacing just the joint surface of the humeral head with a cap-like prosthesis without a stem. With its bone preserving advantage, it offers those with arthritis of the shoulder an alternative to the standard stemmed shoulder replacement.
Resurfacing hemiarthroplasty may be an option for you if:
- The glenoid still has an intact cartilage surface
- There has been no fresh fracture of the humeral neck or head
- There is a desire to preserve humeral bone
For patients who are young or very active, resurfacing hemiarthroplasty avoids the risks of component wear and loosening that may occur with conventional total shoulder replacements in this patient population. Due to its more conservative nature, resurfacing hemiarthroplasty may be easier to convert to total shoulder replacement, if necessary at a later time.

Reverse Total Shoulder Replacement
Another type of shoulder replacement is called reverse total shoulder replacement. Reverse total shoulder replacement is used for people who have:

- Completely torn rotator cuffs with severe arm weakness
- The effects of severe arthritis and rotator cuff tearing (cuff tear arthropathy)
- Had a previous shoulder replacement that failed
For these individuals, a conventional total shoulder replacement can still leave them with pain. They may also be unable to lift their arm up past a 90-degree angle. Not being able to lift one’s arm away from the side can be severely debilitating.
In reverse total shoulder replacement, the socket and metal ball are switched. That means a metal ball is attached to the shoulder bone and a plastic socket is attached to the upper arm bone. This allows the patient to use the deltoid muscle instead of the torn rotator cuff to lift the arm.

Complications
Your orthopaedic surgeon will explain the potential risks and complications of shoulder joint replacement, including those related to the surgery itself and those that can occur over time after your surgery.
When complications occur, most are successfully treatable. Possible complications include the following.
Infection
Infection is a complication of any surgery. In shoulder joint replacement, infection may occur in the wound or deep around the prosthesis. It may happen while in the hospital or after you go home. It may even occur years later. Minor infections in the wound area are generally treated with antibiotics. Major or deep infections may require more surgery and removal of the prosthesis.
Any infection in your body can spread to your joint replacement.
Prosthesis Problems
Although prosthesis designs and materials, as well as surgical techniques, continue to advance, the prosthesis may wear down and the components may loosen. The components of a shoulder replacement may also dislocate. Excessive wear, loosening, or dislocation may require additional surgery (revision procedure).
Nerve Injury
Nerves in the vicinity of the joint replacement may be damaged during surgery, although this type of injury is infrequent. Over time, these nerve injuries often improve and may completely recover.
-
Thank you so much for all your help. Your professional, approachable manner was second to none. With best wishes.
P.J.
-
Many thanks for your care and expertise.
J.F.
-
I would like to take this opportunity to thank you for seeing me so expediently, and for everything that you have done following my scan. Your astute judgement and endeavours in the operating theatre have made this experience painless and have encouraged much optimism and positivity in the rehabilitation period, which is progressing smoothly.
M.H.
All of our practitioners are approved by leading insurance companies

Cookie Policy
This site uses cookies in the interest of providing the best user experience. If you continue without changing your settings, it will be assumed that you are happy to receive all cookies from the andyhenry.co.uk site. If you do not wish to receive cookies from this site, you are free to change your cookie settings at any time.